Care management director
Clinical care coordinator
Primary care physician
Social worker
Population health manager
Nurse case manager

This process is used when a clinical team, provider, or health plan identifies a patient who meets criteria for care management services — such as chronic disease management, transitional care after hospitalization, behavioral health support, or social determinants of health intervention. It applies when the patient’s clinical status, utilization patterns, or social factors indicate that structured care coordination would improve outcomes and reduce avoidable utilization. It is common when referring providers, care management intake teams, and the patient must coordinate to assess eligibility, gather clinical context, and initiate services. Ideal for health systems, managed care organizations, accountable care organizations, and any healthcare entity with population health or care management programs.
The care management referral process typically involves the referring provider or clinical team who identifies the patient and initiates the referral, care management intake coordinators who assess eligibility and triage the referral, care managers or nurse case managers who accept the case and begin care planning, social workers who address non-clinical needs, and the patient who participates in the assessment and consents to services.
Faster time to care management enrollment by routing referrals to the right program based on clinical criteria, acuity, and patient needs. Fewer dropped referrals because every referral is tracked from initiation through enrollment or appropriate disposition. Complete clinical handoff so care managers receive the patient’s clinical history, current medications, care gaps, and social context at intake rather than re-gathering information. Improved patient engagement by involving the patient in the referral process and making it easy for them to participate in the initial assessment. Better population health outcomes because patients who meet care management criteria are identified and enrolled rather than falling through gaps in the referral process.
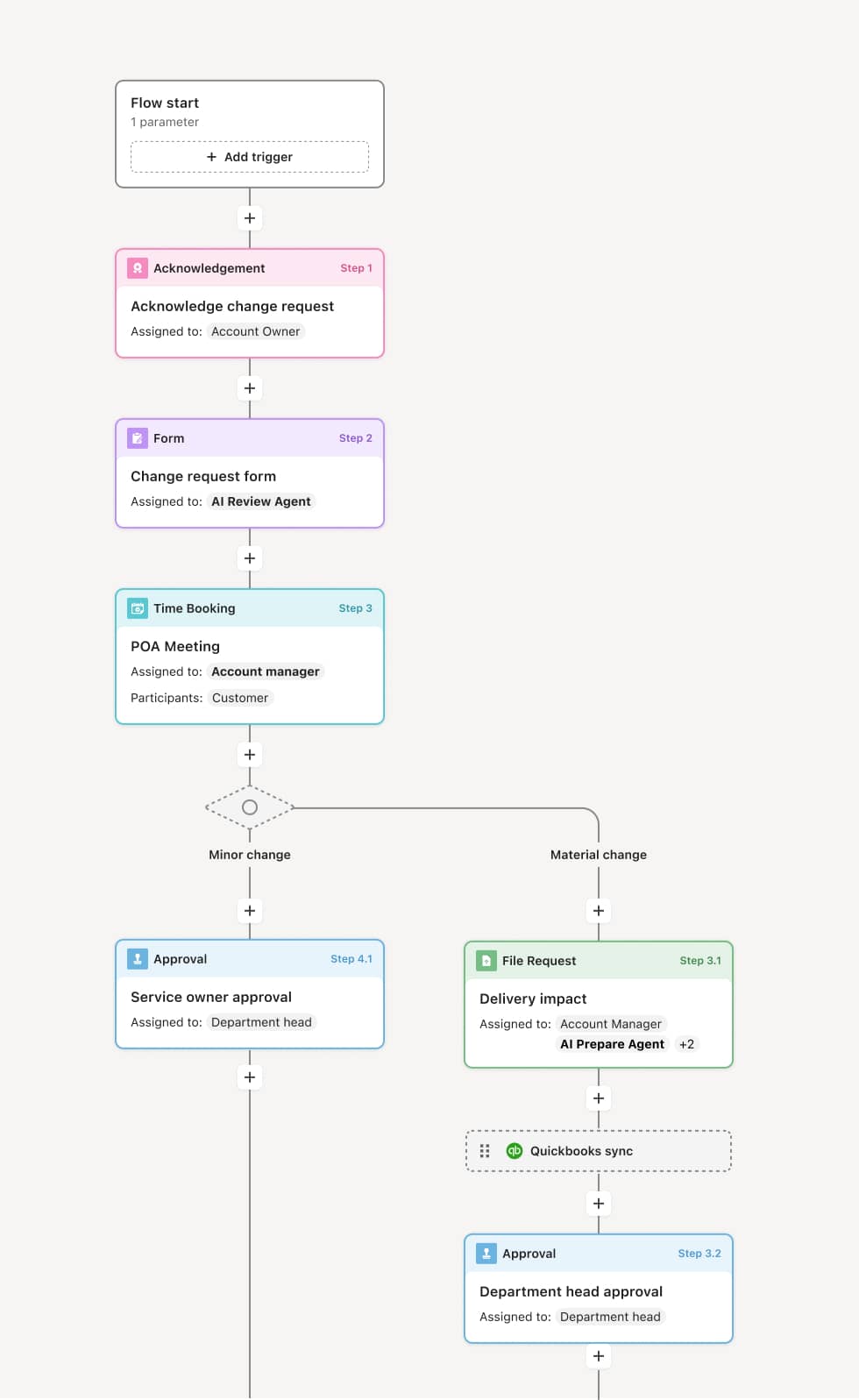
Your version of this process may vary based on roles, systems, data, and approval paths. Moxo’s flow builder can be configured with AI agents, conditional branching, dynamic data references, and sophisticated logic to match how your organization runs this workflow. The steps below illustrate one example.
Referral initiation
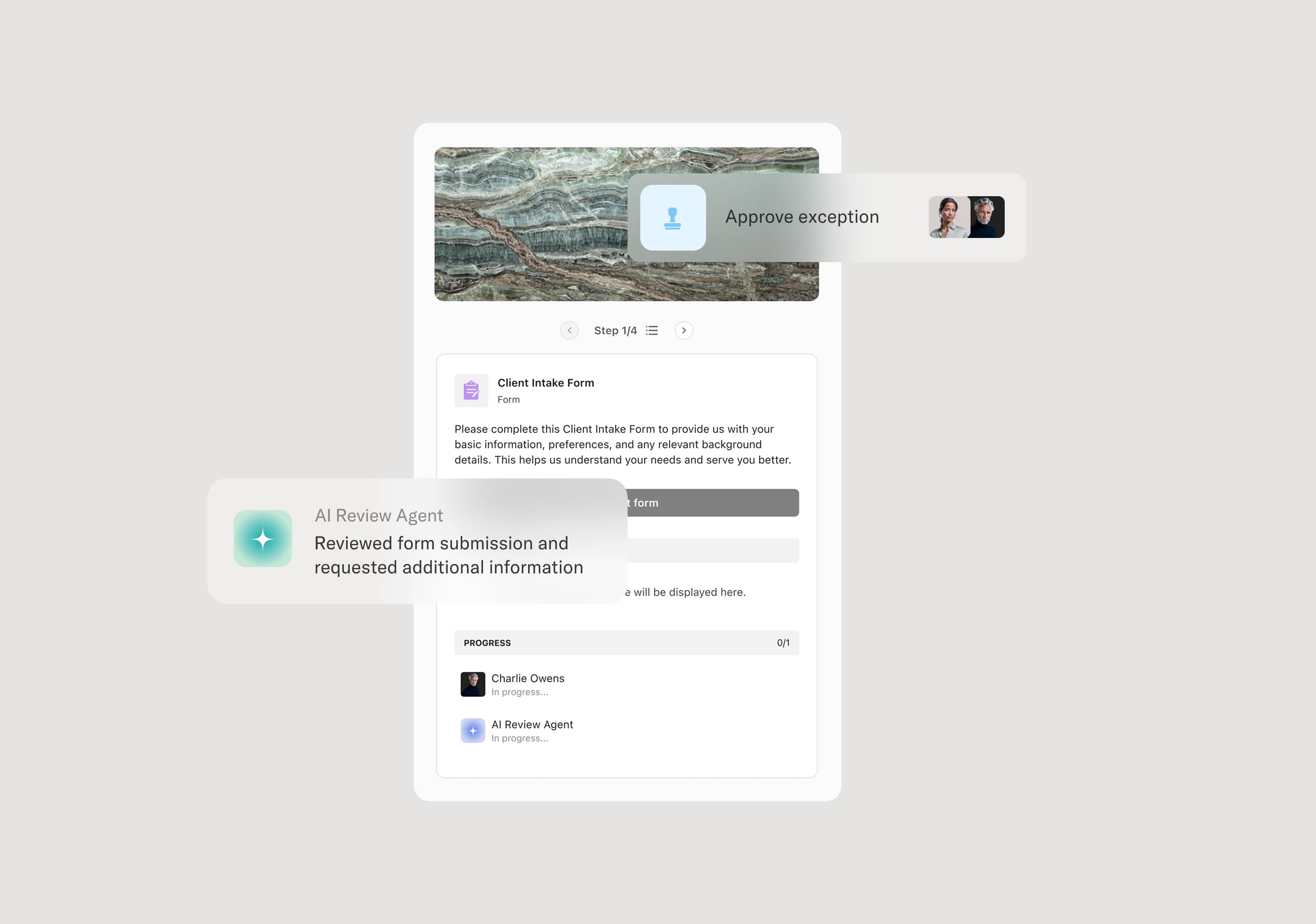
The process begins when a provider, clinical team, or population health system identifies a patient who meets criteria for care management services. The referring party submits a referral that includes the patient’s clinical summary, relevant diagnoses, current medications, recent utilization, and the reason for referral. An AI Agent can assist by validating the referral against program eligibility criteria and flagging missing clinical information before it reaches the care management team.
Intake triage and eligibility assessment
The care management intake team reviews the referral to confirm the patient’s eligibility for the recommended program. This includes assessing acuity level, clinical complexity, and the appropriateness of the program match. If the referral does not meet criteria, it is redirected to a more appropriate service or returned to the referring provider with guidance.
Patient outreach and consent
The care management team contacts the patient to explain the program, discuss their needs, and obtain consent for enrollment. If the patient declines or cannot be reached within defined attempts, the referral is documented with the disposition and the referring provider is notified. An AI Agent may prepare a patient-facing summary of the program and next steps to support the outreach.
Comprehensive assessment
Once the patient consents, the care manager conducts a comprehensive assessment that covers clinical status, medications, functional limitations, behavioral health, social determinants, and care goals. This assessment informs the care plan and determines the level of ongoing coordination required.
Care plan development and assignment
Based on the assessment, the care manager develops an individualized care plan and is formally assigned to the case. The care plan, along with the referral context and assessment findings, is shared with the patient and relevant providers.
Enrollment confirmation and record preservation
The patient is enrolled in the care management program. The referring provider is notified of enrollment. The complete referral record — including clinical context, eligibility assessment, patient consent, comprehensive assessment, and care plan — is preserved for continuity and regulatory compliance.
This process commonly relies on inputs such as the referral form, clinical summary, medication list, utilization data, and patient demographics. It may be triggered by a provider referral, an ED discharge, a health risk assessment, or a population health analytics flag. Connected systems often include EHR platforms like Epic or Cerner for clinical data, care management platforms like Guiding Care or HealthEC, and health information exchanges for cross-provider data sharing.
Key decision points include whether the patient meets the clinical and program eligibility criteria for the referred care management program, whether the patient consents to enrollment and participates in the assessment, which care management program and acuity level best match the patient’s needs, and whether the comprehensive assessment reveals needs that require adjustment to the initial care plan or program assignment.
Referrals submitted without sufficient clinical context, requiring care management to re-gather information and delaying intake. Patients lost during outreach when multiple contact attempts go undocumented and no follow-up process is triggered. Eligibility mismatches when patients are referred to programs that do not match their clinical or social needs, requiring re-routing. Delayed enrollment when administrative steps like consent collection or assessment scheduling are not tracked and followed up. Referring providers not notified of referral outcomes, undermining trust in the care management process.
Orchestrates the referral lifecycle from initiation through enrollment across referring providers, care management intake, and the patient in a single coordinated flow.
Routes referrals based on clinical criteria and program eligibility so patients reach the right care management program without manual triage delays.
AI Agents validate referral completeness at submission, flagging missing clinical data or eligibility gaps before the referral reaches the intake team.
Engages patients directly within the workflow for outreach, consent, and assessment scheduling so every interaction is tracked and context is preserved.
Connects to EHR and care management platforms like Epic, Cerner, and Guiding Care so clinical data and enrollment records stay synchronized.
Preserves the complete referral record including clinical context, eligibility assessment, patient consent, and care plan for continuity, regulatory compliance, and program performance analysis.