CDI program director
Clinical documentation specialist
Health information management director
Physician advisor
Coding supervisor
Revenue integrity manager

This process is used when clinical documentation in the patient record does not fully or accurately reflect the patient’s clinical status, severity of illness, or the complexity of care provided. It applies during concurrent inpatient stays (concurrent CDI review) and retrospectively after discharge (retrospective review), particularly when documentation gaps affect diagnosis-related group (DRG) assignment, risk adjustment, quality metrics, or regulatory compliance. It is common when CDI specialists, attending physicians, coding teams, and quality staff must coordinate to improve documentation before or after final coding. Ideal for hospitals, health systems, and any healthcare organization managing clinical documentation accuracy for coding, reimbursement, and quality reporting.
The CDI process typically involves CDI specialists who review records and identify documentation opportunities, attending physicians who respond to queries and provide documentation clarification, physician advisors who support the CDI program and provide clinical guidance, coding professionals who assess the documentation for coding accuracy, and health information management leaders who oversee the program and report outcomes.
More accurate DRG assignment because documentation reflects the true severity and complexity of the patient’s condition. Improved physician query response rates by routing queries through a structured, trackable workflow rather than paper or informal channels. Better quality metric performance since clinical documentation directly affects publicly reported quality measures and risk-adjusted outcomes. Revenue integrity through documentation that supports the level of care actually provided, reducing under-coding and audit risk. Reduced retrospective corrections because concurrent CDI review catches documentation gaps while the patient is still in-house and the physician has current clinical context.
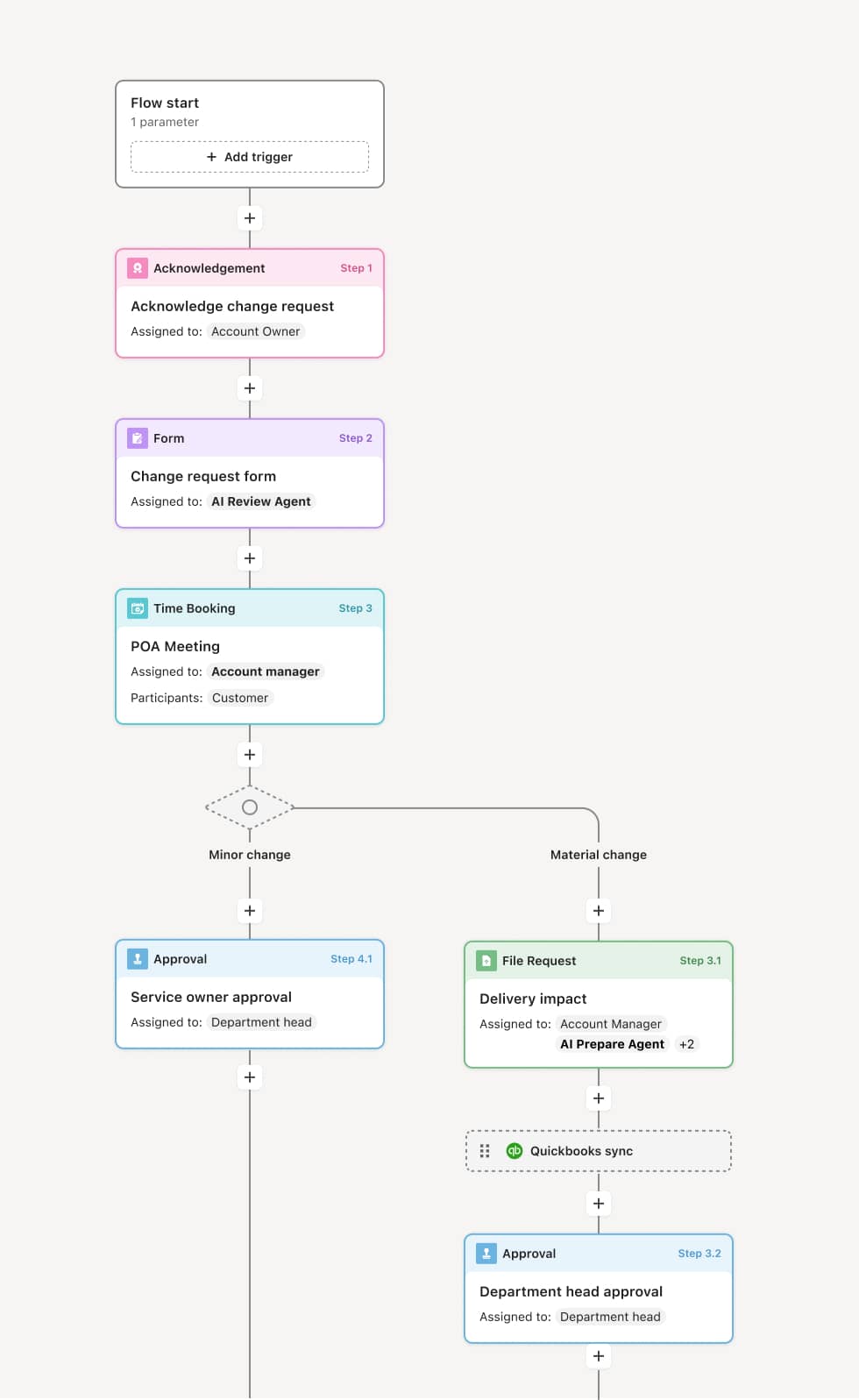
Your version of this process may vary based on roles, systems, data, and approval paths. Moxo’s flow builder can be configured with AI agents, conditional branching, dynamic data references, and sophisticated logic to match how your organization runs this workflow. The steps below illustrate one example.
Record review and opportunity identification
The process begins when a CDI specialist reviews the patient’s clinical record — typically within the first 24 to 48 hours of an inpatient admission. The specialist evaluates whether the documentation accurately reflects the patient’s principal diagnosis, comorbidities, severity of illness, and risk of mortality. An AI Agent can assist by scanning the record for common documentation gaps, such as unspecified diagnoses, missing clinical indicators, or conditions documented in nursing notes but not in physician orders.
Physician query generation
When a documentation gap is identified, the CDI specialist generates a compliant physician query — a non-leading, clinically supported request for the physician to clarify, confirm, or add documentation. Queries may address topics such as the clinical significance of abnormal lab values, the specificity of a diagnosis, or the presence of conditions supported by clinical evidence but not yet documented. An AI Agent may suggest query templates based on the type of documentation opportunity.
Physician response and documentation update
The attending physician receives the query and provides a response — either through an addendum to the medical record, a verbal clarification documented by the CDI specialist, or a direct update in the EHR. If the physician does not respond within the expected timeframe, the query is escalated or resubmitted. The CDI specialist confirms that the documentation update addresses the original query.
Coding alignment review
After the documentation is updated, the coding team reviews the record to confirm that the assigned codes now accurately reflect the clinical documentation. If additional documentation is still needed to support a code, a follow-up query may be generated. The CDI specialist and coder reconcile any discrepancies between the clinical and coding perspectives.
Final documentation assessment
At discharge or final coding, the complete record is assessed for documentation accuracy and coding alignment. The CDI review findings, queries, physician responses, and coding outcomes are documented as part of the case record.
Program reporting and education
CDI outcomes are aggregated for program reporting, including query rates, response rates, DRG impact, and documentation improvement trends. Results inform physician education priorities and CDI program strategy.
This process commonly relies on inputs such as the inpatient clinical record, physician orders, nursing assessments, laboratory and imaging results, and current coding data. It may be triggered by an admission event, a DRG-based worklist, or a retrospective audit queue. Connected systems often include EHR platforms like Epic or Cerner for clinical records, CDI workflow tools like 3M 360 Encompass or Optum CDI, and encoder/grouper systems for DRG analysis.
Key decision points include whether the clinical documentation accurately reflects the patient’s severity of illness and complexity of care, which documentation gaps warrant a physician query versus those that can be resolved through other means, whether the physician’s response adequately addresses the documentation opportunity, and whether the updated documentation aligns with accurate code assignment.
Queries not reaching physicians promptly, especially in settings where paper-based or informal query methods are used. Low physician response rates that leave documentation gaps unresolved before discharge and final coding. Non-compliant query language that leads to audit findings if queries are leading, presumptive, or not clinically supported. CDI reviews initiated too late in the admission, missing the window for concurrent documentation improvement. Program metrics not tracked, making it difficult to demonstrate CDI impact on documentation quality, reimbursement, and quality reporting.
Orchestrates the CDI review cycle from record review through physician query, response, and coding alignment across CDI specialists, physicians, and coding teams in a single workflow.
Routes physician queries directly to the attending provider with clinical context and tracking, improving response rates compared to paper or informal channels.
AI Agents scan clinical records for documentation gaps and suggest query opportunities, accelerating the CDI specialist’s review process.
Tracks query response timelines and escalates unanswered queries to ensure documentation is updated before discharge and final coding.
Connects to EHR and CDI platforms like Epic, Cerner, and 3M 360 Encompass so clinical data, queries, and coding records are accessible in context.
Captures CDI program metrics including query rates, response rates, DRG impact, and documentation trends for program management, physician education, and executive reporting.