Utilization management director
Clinical reviewer
Medical director
Case management coordinator
Payer operations lead
Quality improvement manager

This process is used when a healthcare service, admission, continued stay, or procedure requires evaluation to determine whether it meets medical necessity criteria and is appropriate for the proposed level of care. It applies across three review types: prospective (before the service), concurrent (during an inpatient stay), and retrospective (after the service). It is common when clinical reviewers, medical directors, and treating providers must coordinate to assess clinical information against established criteria such as InterQual or Milliman. Ideal for health plans, managed care organizations, hospitals, and utilization review organizations.
The utilization management process typically involves clinical reviewers (nurses) who perform initial clinical evaluation against criteria, medical directors who make determinations when cases do not meet initial criteria, treating providers who supply clinical information and may request reconsideration, case managers who coordinate care transitions, and UM coordinators who manage the review workflow and documentation.
Clinically appropriate utilization decisions because every review is evaluated against evidence-based criteria with physician oversight for adverse determinations. Timely review turnaround that meets NCQA, state, and CMS requirements for prospective, concurrent, and urgent review timelines. Reduced unnecessary utilization through consistent application of medical necessity criteria. Protected patient access because denials include clear clinical rationale, appeal rights, and alternative care recommendations. Complete UM documentation supporting audit, accreditation, regulatory compliance, and quality improvement.
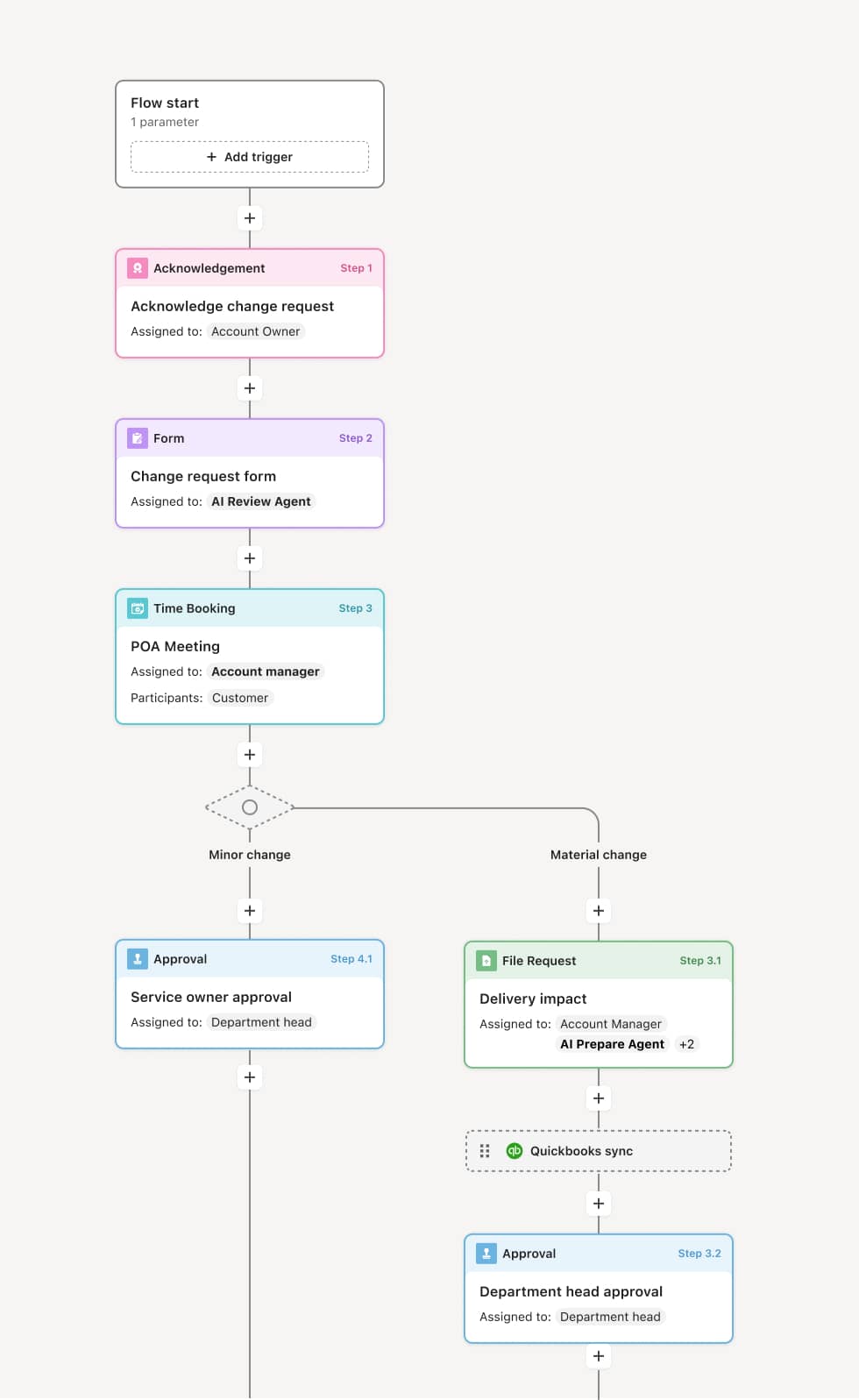
Your version of this process may vary based on roles, systems, data, and approval paths. Moxo’s flow builder can be configured with AI agents, conditional branching, dynamic data references, and sophisticated logic to match how your organization runs this workflow. The steps below illustrate one example.
Review request receipt
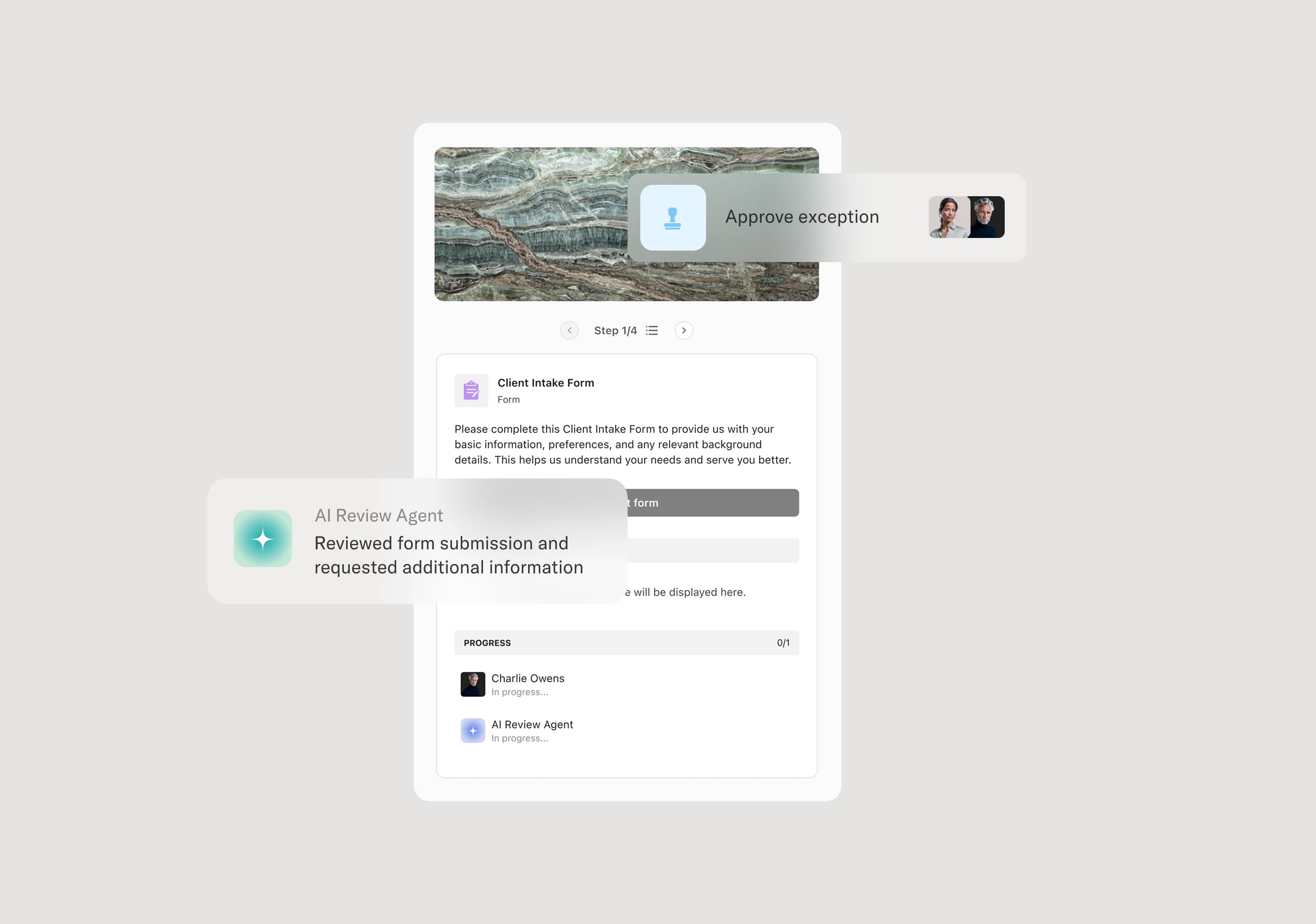
The process begins when a utilization review request is received — a prior authorization for a planned service, a continued stay review for an inpatient, or a post-service review. The request includes the patient’s clinical information, the proposed service, and the treating provider’s rationale. An AI Agent can assist by extracting key clinical data and identifying the appropriate review criteria.
Initial clinical review
A clinical reviewer evaluates the request against established clinical criteria such as InterQual or Milliman Care Guidelines. If the request meets criteria, it is approved and the treating provider is notified. If the request does not clearly meet criteria, the case is referred to the medical director.
Medical director review
The medical director reviews cases that did not meet criteria at the initial clinical review. The medical director may request additional clinical information, consult with the provider directly (peer-to-peer), or make a determination based on available information. If denied, the denial includes the clinical rationale and the patient’s and provider’s appeal rights.
Provider communication and peer-to-peer review
When additional clinical information is needed or the provider disagrees with a preliminary determination, a peer-to-peer discussion is offered. The treating provider and medical director discuss the clinical details. An AI Agent may prepare the case summary for the peer-to-peer discussion.
Determination and notification
The final determination is communicated to the treating provider and the patient within the required turnaround timeframe. Denials include the specific clinical rationale, the criteria applied, and instructions for appeal.
Concurrent review and continued stay management
For inpatient concurrent reviews, the process repeats at defined intervals to reassess continued medical necessity. Each review evaluates whether the patient’s clinical status supports continued stay at the current level of care or whether a transition is appropriate.
This process commonly relies on inputs such as the clinical review request, patient medical records, treating provider’s rationale, clinical review criteria (InterQual, Milliman), and payer benefit information. It may be triggered by a prior authorization request, an inpatient admission notification, or a retrospective review queue. Connected systems often include UM platforms with decision support, care management platforms, EHR systems, and payer claims systems.
Key decision points include whether the requested service meets clinical criteria at the initial nursing review level, whether the medical director approves or denies services that do not meet initial criteria, whether a peer-to-peer review provides additional justification that changes the determination, and whether continued stay reviews support ongoing inpatient care or indicate readiness for transition.
Insufficient clinical information submitted with the review request, requiring back-and-forth that delays the determination. Review turnaround times exceeded because cases are not triaged by urgency. Medical director review bottleneck when the volume of referred cases exceeds available physician reviewer capacity. Denial letters lacking specific clinical rationale, creating compliance risk. Concurrent reviews not conducted at required intervals, missing opportunities to manage length of stay.
Orchestrates utilization review across clinical reviewers, medical directors, and treating providers in a single workflow that manages prospective, concurrent, and retrospective reviews.
Routes cases based on review type and clinical determination so approvals are processed quickly while cases requiring physician review reach the medical director promptly.
AI Agents extract clinical data from review requests and match it against applicable criteria, accelerating the initial clinical review.
Facilitates peer-to-peer review scheduling and documentation within the workflow so provider discussions are tracked and incorporated into the determination.
Tracks review turnaround times against NCQA, state, and CMS requirements, alerting the team when deadlines are approaching.
Preserves the complete UM record including clinical reviews, determinations, denial rationale, peer-to-peer notes, and appeal documentation for accreditation, audit, and quality analysis.