Coding supervisor
Health information management director
Clinical documentation improvement specialist
Revenue integrity manager
Compliance officer
Medical coder

This process is used when coded encounters require review before claim submission to verify accuracy, completeness, and compliance with ICD-10, CPT, HCPCS, and payer-specific coding guidelines. It applies to high-complexity encounters, high-value procedures, new coders’ work requiring quality checks, encounters flagged by coding edits, and random audit samples for compliance monitoring. It is common when coders, clinical documentation specialists, and coding supervisors must coordinate to validate that codes reflect the clinical record. Ideal for hospitals, physician practices, ambulatory surgery centers, and any healthcare organization managing coded claims for reimbursement.
The medical coding review process typically involves medical coders who assign initial codes based on the clinical documentation, clinical documentation improvement (CDI) specialists who query providers for documentation clarification, coding supervisors or auditors who review coded encounters for accuracy, compliance officers who oversee coding audit programs, and billing staff who depend on accurate codes for clean claim submission.
Higher first-pass claim acceptance rates because coding errors and documentation gaps are caught before submission. Reduced denial and audit risk through pre-submission validation of code accuracy and documentation support. Improved coding consistency across the coding team through structured review, feedback, and education. Faster revenue realization because clean claims reach payers without coding-related holds or rejections. Documented coding quality metrics that support compliance programs, audit readiness, and coder performance management.
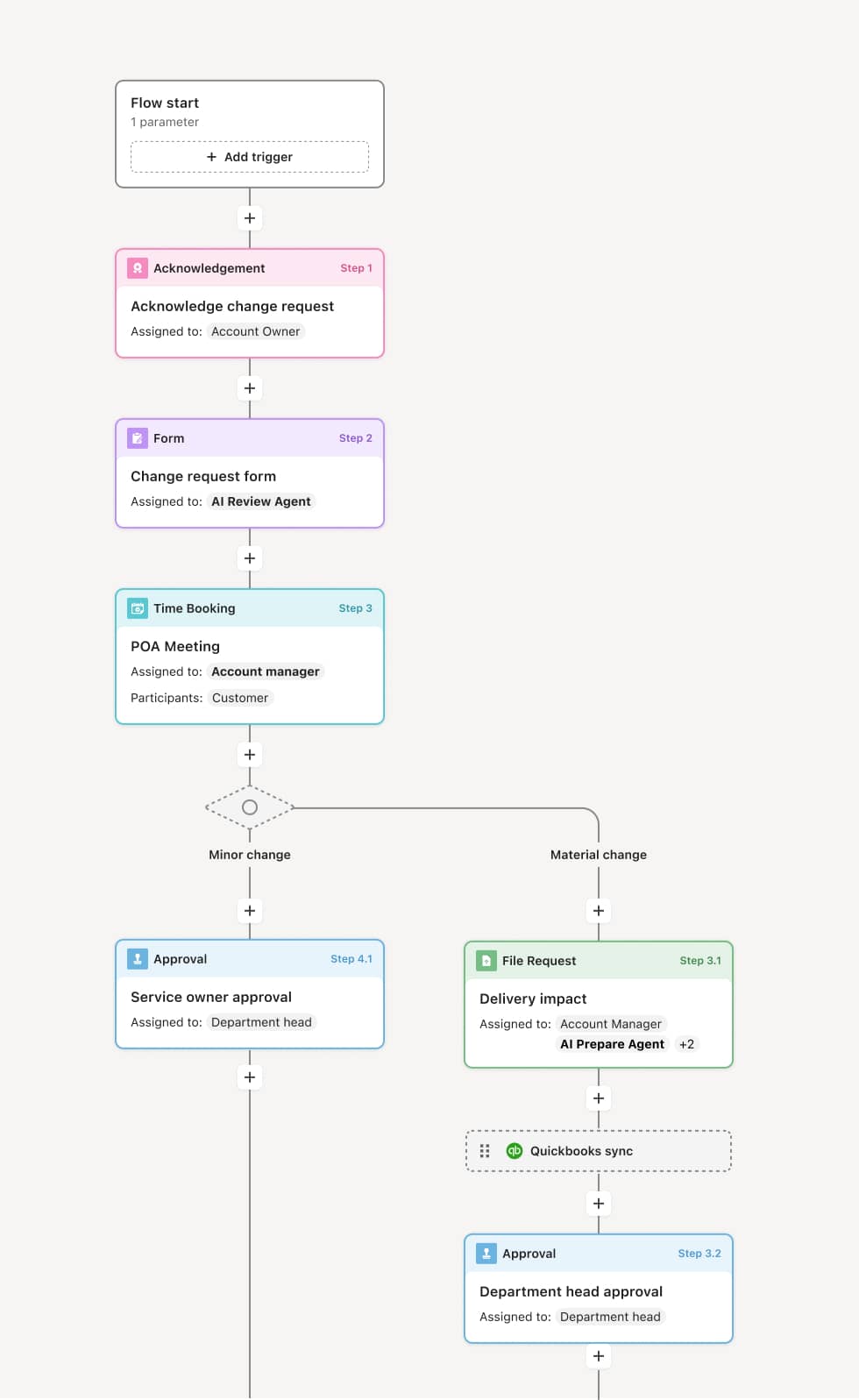
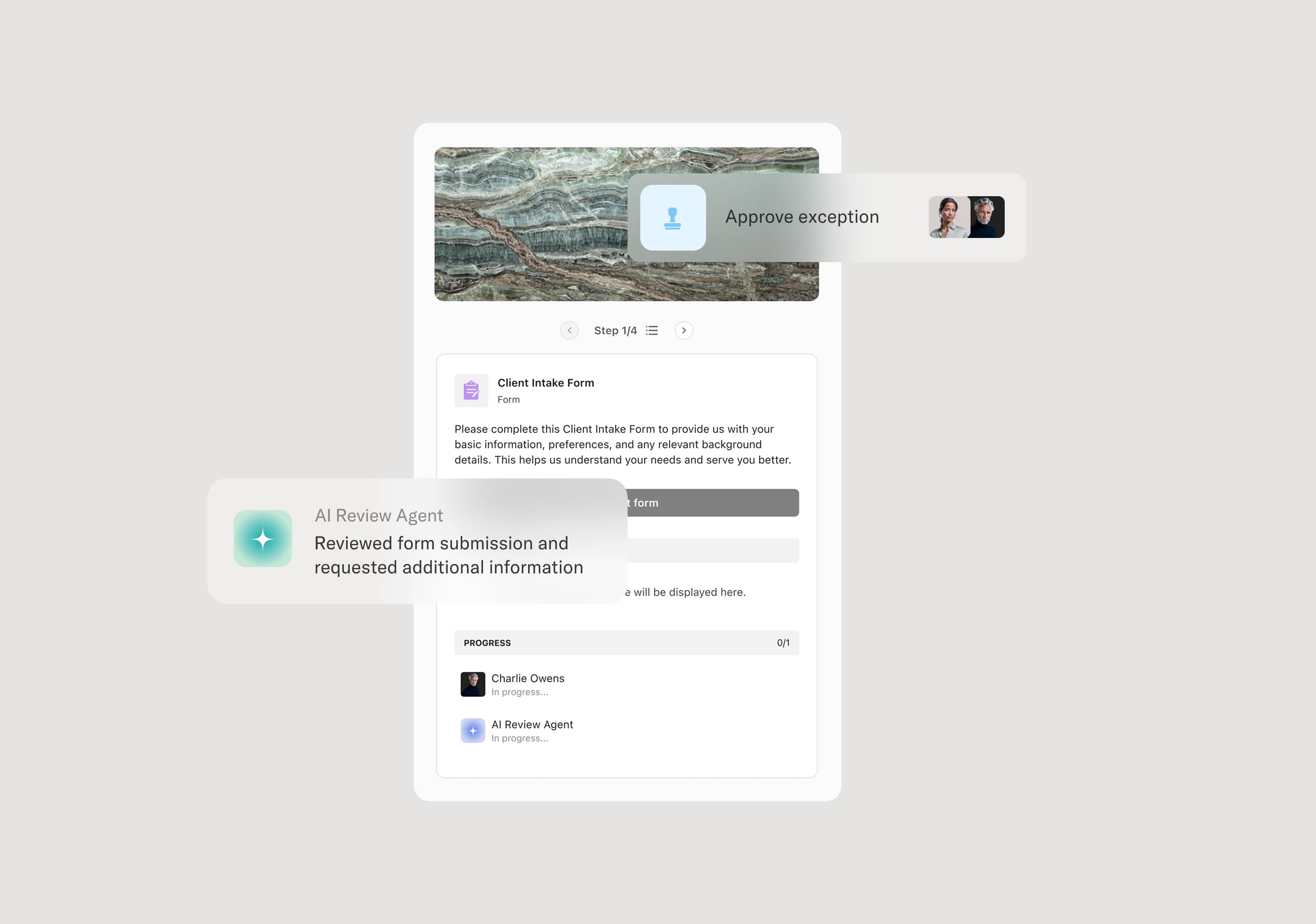
Your version of this process may vary based on roles, systems, data, and approval paths. Moxo’s flow builder can be configured with AI agents, conditional branching, dynamic data references, and sophisticated logic to match how your organization runs this workflow. The steps below illustrate one example.
Encounter coding completion
The process begins when a medical coder completes the initial coding of a patient encounter, assigning diagnostic codes (ICD-10), procedure codes (CPT/HCPCS), and modifiers based on the clinical documentation. The coded encounter enters the review queue based on the organization’s review criteria — such as encounter complexity, procedure type, coder experience level, or random audit selection.
Documentation sufficiency check
A clinical documentation improvement specialist or coding reviewer assesses whether the clinical documentation adequately supports the assigned codes. If documentation gaps exist — such as unspecified diagnoses, missing clinical indicators, or insufficient procedure detail — a provider query is generated to request clarification before the review proceeds. An AI Agent may flag common documentation deficiency patterns based on the encounter type and assigned codes.
Code accuracy and compliance review
The coding supervisor or auditor reviews the assigned codes against the clinical record, coding guidelines, payer-specific rules, and applicable edits. The review evaluates whether codes are accurate, specific, complete, and compliant with national and local coverage determinations. If errors are identified, the codes are returned to the original coder with specific feedback and correction instructions.
Feedback and correction
The coder reviews the feedback, makes corrections, and resubmits the encounter. If the coder disagrees with the reviewer’s assessment, a discussion or escalation process is available to resolve the discrepancy. This feedback loop supports continuous coder education and quality improvement.
Final validation and release to billing
Once the coded encounter passes review, it is validated and released for claim submission. The review results, including any corrections, queries, and feedback, are documented as part of the coding quality record.
Quality reporting and trend analysis
Coding review results are aggregated for quality reporting — tracking error rates by coder, code category, encounter type, and documentation source. These metrics inform targeted education, process improvements, and compliance program priorities.
This process commonly relies on inputs such as the coded encounter record, clinical documentation (physician notes, operative reports, discharge summaries), coding guidelines, payer-specific edits, and audit selection criteria. It may be triggered by encounter complexity flags, random audit schedules, or coding edit failures. Connected systems often include coding and encoder platforms like 3M or Optum, EHR platforms like Epic or Cerner for clinical records, and billing systems for claim submission.
Key decision points include whether the encounter meets criteria for pre-submission coding review, whether the clinical documentation sufficiently supports the assigned codes or requires a provider query, whether identified coding errors are corrected before the encounter is released to billing, and whether coding quality trends warrant targeted education or process changes.
Documentation queries not returned promptly by providers, delaying coding completion and claim submission. Inconsistent review criteria that result in some high-risk encounters being released without review. Coder feedback not actionable, providing general comments instead of specific guidance tied to coding rules and documentation. Review bottlenecks when coding supervisors cannot keep pace with the volume of encounters requiring quality checks. Quality data not used for improvement, allowing recurring coding errors to persist without targeted education or process correction.
Orchestrates coding review across coders, CDI specialists, coding supervisors, and billing in a single workflow that keeps encounters moving toward clean claim submission.
Routes encounters for review based on complexity, procedure type, coder experience, and audit criteria so high-risk encounters receive appropriate scrutiny.
AI Agents flag documentation gaps and common coding patterns at the point of review, accelerating the identification of issues that would cause denials.
Manages the provider query process within the workflow so documentation requests and responses are tracked and tied to the specific encounter.
Connects to coding platforms, EHR systems, and billing tools like 3M, Epic, and Athenahealth so clinical records, coded data, and claim status are accessible in context.
Captures coding quality metrics for every reviewed encounter, supporting coder education, compliance reporting, and continuous improvement in coding accuracy.