Medical director
Clinical reviewer
Utilization management lead
Payer medical officer
Treating physician
Clinical appeals specialist

This process is used when a proposed service, procedure, admission, or treatment requires a determination of medical necessity before the payer will authorize coverage. It applies when the treating provider’s clinical justification must be evaluated against established criteria — such as InterQual, Milliman, or payer-specific clinical policies — to determine whether the proposed care is appropriate for the patient’s condition, setting, and level of service. It is common when clinical reviewers, medical directors, and treating providers must coordinate on complex or ambiguous cases. Ideal for health plans, managed care organizations, utilization review organizations, and healthcare systems managing medical necessity determinations.
The medical necessity review process typically involves clinical reviewers (nurses) who perform the initial criteria-based assessment, medical directors who review cases that do not meet criteria at initial review, treating providers who present the clinical justification for the proposed service, payer operations staff who manage the review workflow, and patient advocates or appeals specialists who support the patient if the service is denied.
Evidence-based coverage decisions because every determination is evaluated against published clinical criteria with physician oversight for adverse decisions. Transparent rationale communicated to providers and patients so the basis for the determination is clear and actionable. Faster review turnaround by routing straightforward cases through initial clinical review and escalating only complex or ambiguous cases to the medical director. Reduced inappropriate denials because the review process includes peer-to-peer discussion before finalizing adverse determinations. Complete review documentation that supports appeal, audit, accreditation, and quality improvement activities.
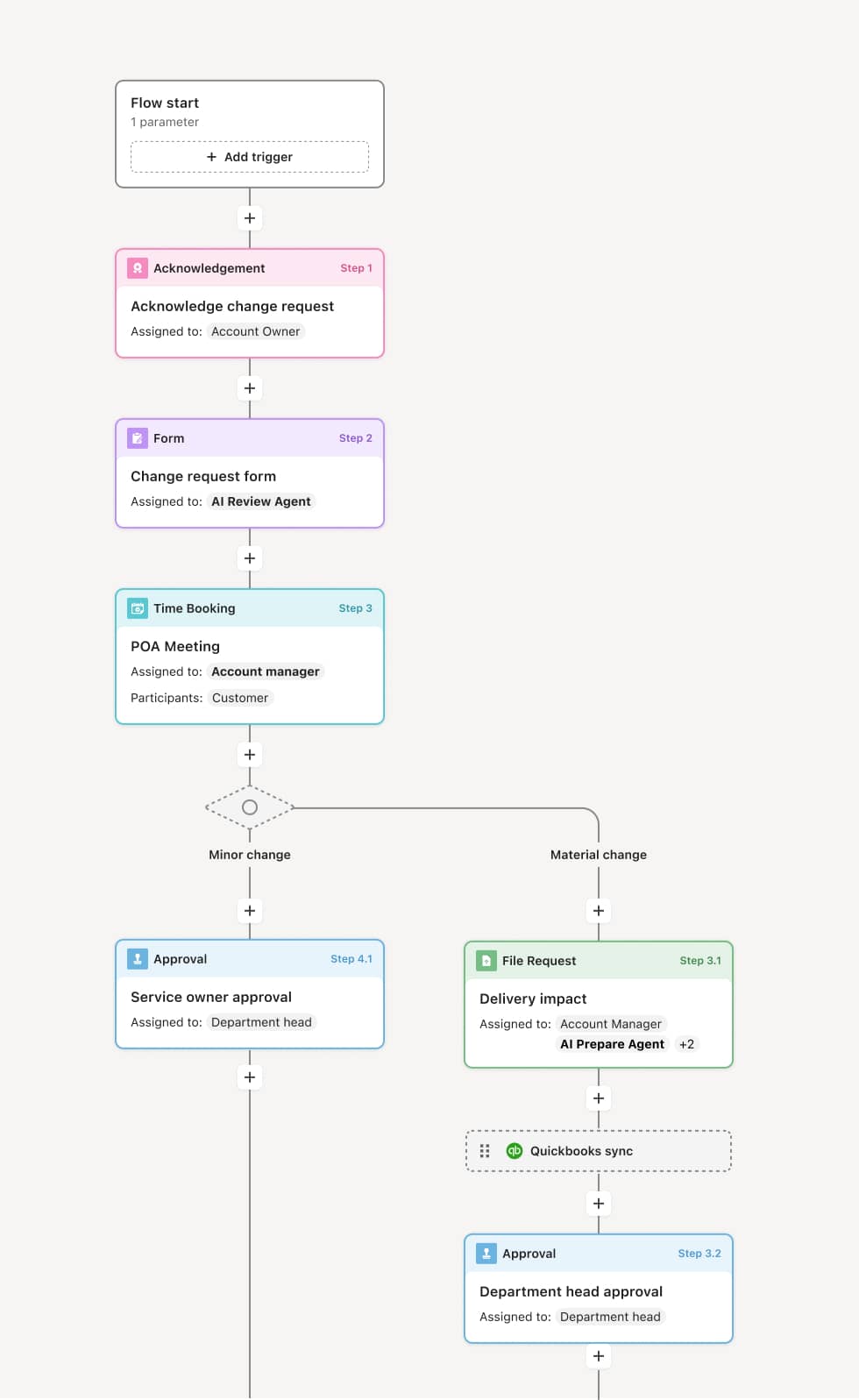
Your version of this process may vary based on roles, systems, data, and approval paths. Moxo’s flow builder can be configured with AI agents, conditional branching, dynamic data references, and sophisticated logic to match how your organization runs this workflow. The steps below illustrate one example.
Review request and clinical data assembly
The process begins when a medical necessity review is triggered by a prior authorization request, a concurrent stay review, or a retrospective claim review. The clinical information is assembled, including the diagnosis, treatment plan, clinical notes, diagnostic results, and the treating provider’s rationale. An AI Agent can assist by extracting key clinical indicators from the submitted documentation and identifying the applicable review criteria.
Initial criteria-based review
A clinical reviewer evaluates the clinical information against the applicable medical necessity criteria. If the proposed service clearly meets criteria, the review is approved. If the clinical information does not meet criteria or is ambiguous, the case is escalated to the medical director for physician-level review.
Medical director evaluation
The medical director reviews the clinical details, applying medical judgment to cases that do not clearly meet criteria. The medical director may request additional information from the treating provider, offer a peer-to-peer discussion, or make a determination based on the available evidence. An AI Agent may surface relevant clinical guidelines, published literature, or prior similar determinations to inform the review.
Peer-to-peer discussion
Before finalizing an adverse determination, the medical director offers the treating provider a peer-to-peer discussion. During this discussion, the provider can present additional clinical context, and the medical director can ask clarifying questions. The outcome of the discussion informs the final determination.
Determination and communication
The final determination — approval, partial approval, or denial — is communicated to the treating provider and the patient. Denials include the specific clinical rationale, the criteria applied, and the patient’s and provider’s appeal rights as required by regulation.
Documentation and quality tracking
The complete review record — including clinical data, criteria applied, reviewer determination, peer-to-peer notes, and final decision — is preserved. Determination patterns are tracked for quality analysis, inter-rater reliability assessment, and compliance reporting.
This process commonly relies on inputs such as the clinical review request, patient medical records, treating provider’s rationale, clinical review criteria (InterQual, Milliman, or payer-specific policies), and benefit plan information. It may be triggered by a prior authorization request, an inpatient review, or a retrospective claim review. Connected systems often include UM platforms with clinical decision support, EHR systems for clinical data, and payer claims and authorization systems.
Key decision points include whether the proposed service meets criteria at the initial clinical review level, whether the medical director approves, requests additional information, or proceeds to an adverse determination, whether the peer-to-peer discussion provides additional clinical context that changes the determination, and whether the denial rationale is specific, defensible, and communicated with required appeal information.
Insufficient clinical information submitted with the review request, requiring multiple rounds of follow-up before the determination can be made. Criteria applied inconsistently across reviewers, creating variation in medical necessity determinations for similar cases. Peer-to-peer discussions not offered before adverse determinations, weakening the determination’s defensibility on appeal. Denial rationale too generic, failing to explain why the specific clinical facts do not meet the specific criteria. Determination patterns not monitored for quality and consistency, allowing inappropriate denial rates to go unaddressed.
Orchestrates medical necessity review across clinical reviewers, medical directors, and treating providers in a single workflow that ensures every case receives appropriate evaluation.
Routes cases based on initial review outcome so approvals are processed quickly while complex cases reach the medical director for physician-level assessment.
AI Agents extract clinical indicators from submitted documentation and identify the applicable criteria, accelerating the initial review.
Coordinates peer-to-peer discussions by scheduling the conversation and providing both physicians with the case summary and criteria within the workflow.
Tracks review turnaround times and determination patterns for quality reporting, inter-rater reliability analysis, and compliance monitoring.
Preserves the complete review record including clinical data, criteria applied, determinations, peer-to-peer notes, and appeal documentation for accreditation, audit, and quality improvement.