Case management director
Discharge planning coordinator
Social worker
Attending physician
Nurse manager
Transitional care lead

This process is used when a hospitalized patient is approaching readiness for discharge and requires coordination of post-acute services, medication management, follow-up appointments, patient education, and transition to home, skilled nursing, rehabilitation, or another care setting. It applies when the discharge plan must account for the patient’s clinical status, functional abilities, social support, insurance coverage, and post-discharge care requirements. It is common when physicians, nurses, case managers, social workers, pharmacy, and external providers must align on the discharge timeline and care transition plan. Ideal for hospitals, health systems, rehabilitation facilities, and any inpatient care setting managing patient transitions.
The discharge planning process typically involves the attending physician who determines medical readiness for discharge, case managers or discharge planners who coordinate post-discharge services and placements, social workers who assess social needs and arrange community resources, bedside nurses who provide discharge education, pharmacists who reconcile medications, and external facilities or home health agencies who receive the patient.
Safer care transitions because discharge plans address clinical, medication, functional, and social needs before the patient leaves the hospital. Reduced readmissions through proactive arrangement of follow-up care, medication reconciliation, and support services. Shorter length of stay by beginning discharge planning at or before admission rather than waiting until the patient is medically ready. Better patient and family preparedness because discharge education, medication instructions, and care plans are communicated before transition. Coordinated handoffs to post-acute providers with complete clinical information and care instructions.
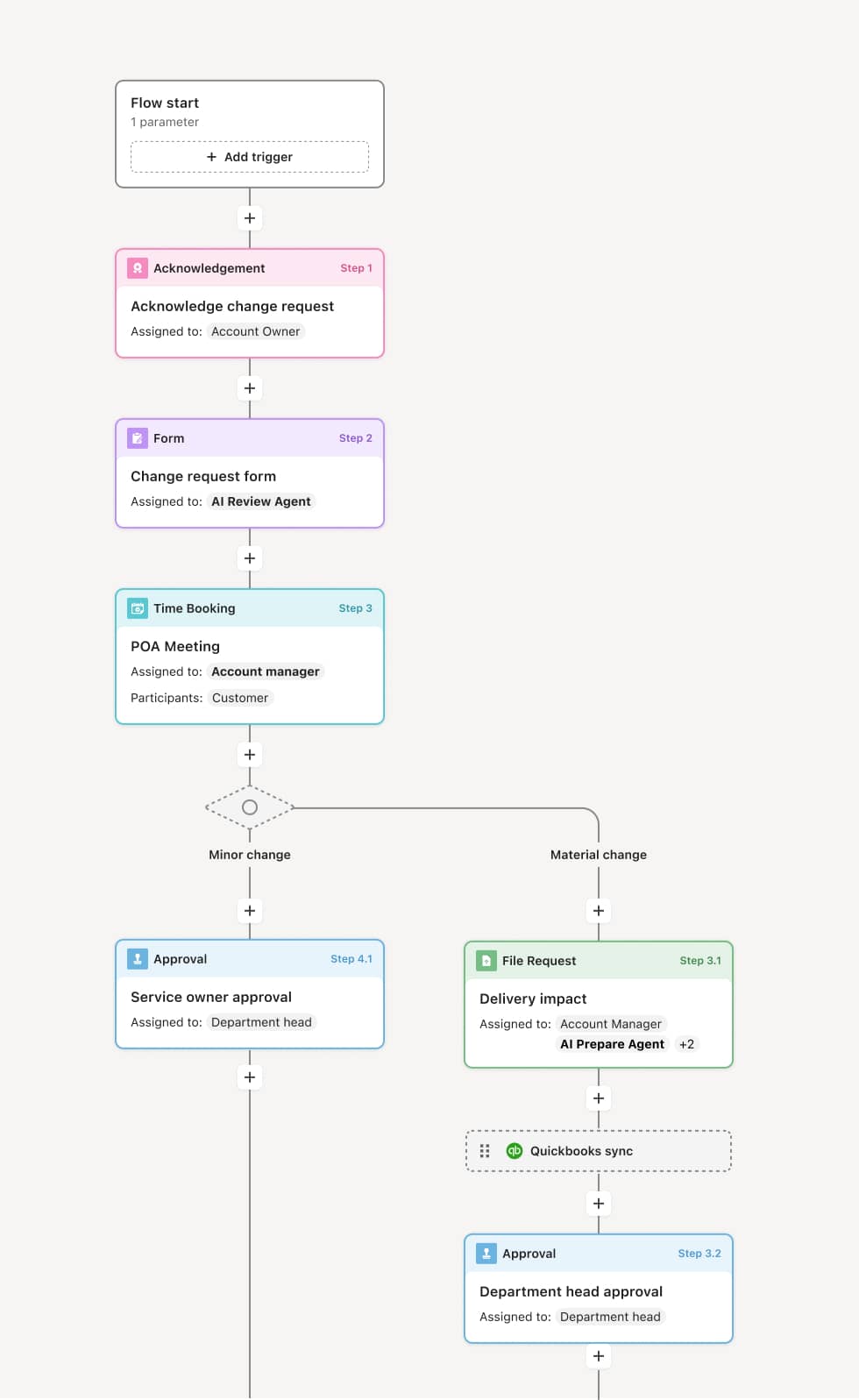
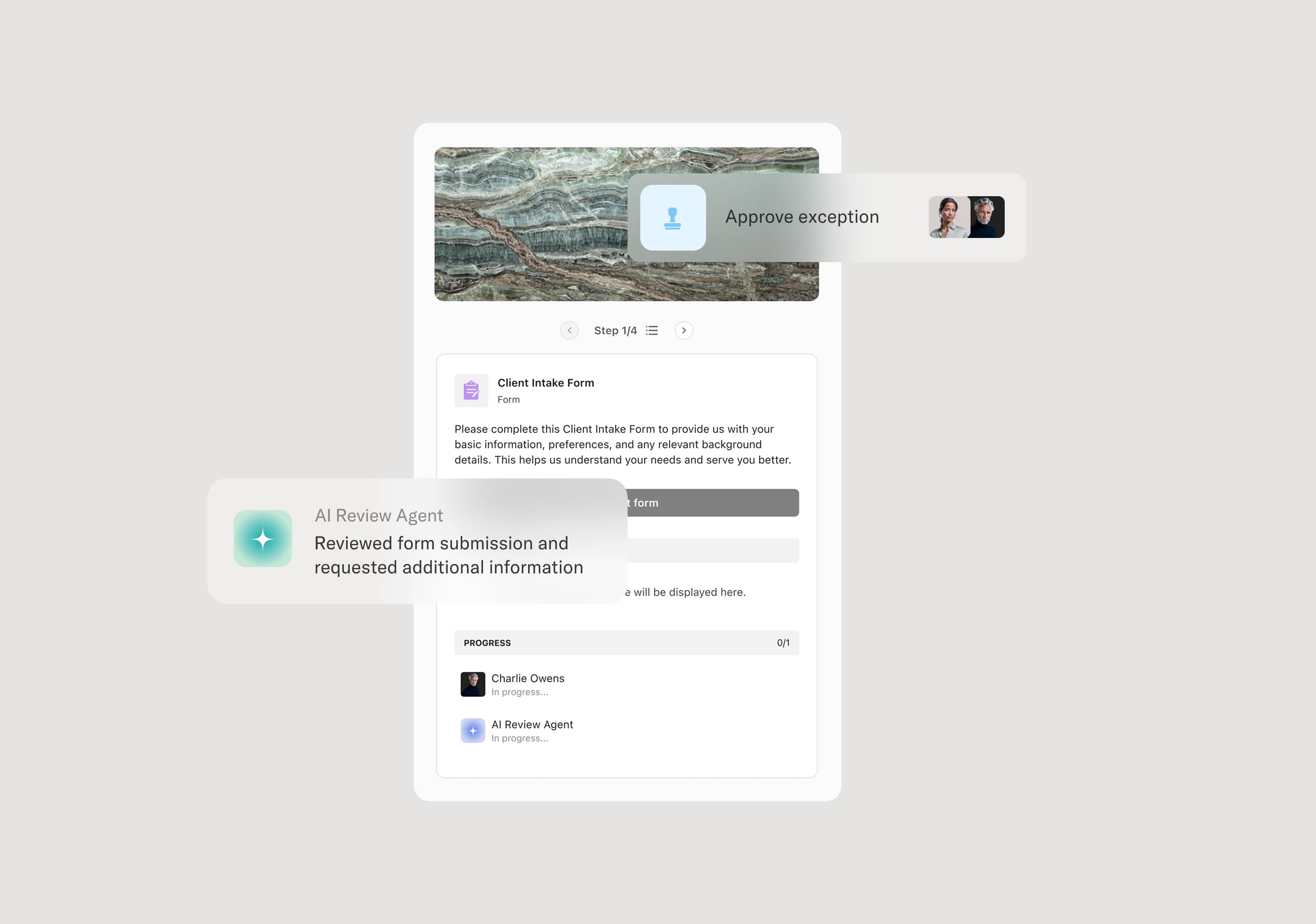
Your version of this process may vary based on roles, systems, data, and approval paths. Moxo’s flow builder can be configured with AI agents, conditional branching, dynamic data references, and sophisticated logic to match how your organization runs this workflow. The steps below illustrate one example.
Early discharge assessment
The process begins at or shortly after admission when the case manager conducts an initial assessment of the patient’s anticipated discharge needs. This includes reviewing the patient’s medical condition, functional status, living situation, social support, insurance coverage, and any known barriers to discharge. An AI Agent can assist by pulling admission data, prior utilization history, and social determinants information to prepare the case manager’s initial assessment.
Care team collaboration and planning
The case manager, social worker, bedside nurse, and attending physician collaborate to develop the discharge plan. This includes identifying the target discharge disposition (home, skilled nursing, rehabilitation, long-term care), required post-discharge services, and any barriers that must be resolved. If the patient requires placement at an external facility, referrals are initiated early.
Medication reconciliation
The pharmacist reviews the patient’s medication regimen, reconciling inpatient medications with pre-admission medications and the discharge medication list. Any changes, new medications, or discontinued medications are documented, and patient education materials are prepared. An AI Agent may flag potential drug interactions, high-risk medications, or insurance formulary issues that could affect post-discharge medication access.
Post-discharge service arrangement
The case manager and social worker arrange post-discharge services based on the plan — home health, durable medical equipment, outpatient therapy, home infusion, community support services, or transportation. Insurance authorizations are obtained where required. Follow-up appointments are scheduled with the primary care provider and relevant specialists.
Patient and family education
The bedside nurse, case manager, or health educator provides discharge education to the patient and family — covering medications, activity restrictions, wound care, warning signs, follow-up appointments, and when to seek emergency care. The patient’s understanding is assessed and documented.
Discharge execution and handoff
On the day of discharge, the attending physician writes the discharge order. The patient receives discharge paperwork, medications, and any required equipment. The clinical summary is transmitted to the receiving provider or facility. The patient is transitioned from the inpatient setting.
Post-discharge follow-up
The care team or transitional care program contacts the patient within a defined window after discharge to assess the transition, address concerns, and confirm that follow-up appointments, medications, and services are in place.
This process commonly relies on inputs such as the patient’s clinical record, functional assessment, insurance coverage details, medication list, social needs assessment, and referral acceptance from post-acute providers. It may be triggered by admission, a clinical milestone, or a physician’s discharge readiness determination. Connected systems often include EHR platforms like Epic or Cerner, care management platforms, pharmacy systems for medication reconciliation, and referral management systems for post-acute coordination.
Key decision points include the target discharge disposition based on the patient’s clinical and functional status, whether the patient requires post-acute services and which services are appropriate, whether insurance authorization is obtained for required post-discharge services, and whether the patient and family demonstrate understanding of the discharge plan and care instructions.
Discharge planning started too late, resulting in extended length of stay while post-discharge services are arranged. Medication reconciliation incomplete at discharge, creating medication errors or access problems after the patient leaves. Post-acute placement delays when referrals are not initiated early or when insurance authorization takes longer than expected. Insufficient patient education that leaves the patient unprepared for self-management at home. Follow-up appointments not confirmed before discharge, contributing to gaps in post-hospital care and potential readmission.
Orchestrates discharge planning from admission assessment through post-discharge follow-up across physicians, case managers, social workers, nurses, pharmacy, and external providers in a single coordinated flow.
Initiates discharge planning early by triggering the assessment workflow at admission rather than waiting for medical readiness.
AI Agents prepare the initial discharge assessment by pulling admission data, utilization history, and social determinants information for the case manager.
Coordinates post-acute referrals and service arrangements within the workflow so external facilities, home health agencies, and equipment providers are engaged and tracked.
Connects to EHR, care management, and pharmacy systems like Epic, Cerner, and referral management platforms so clinical data, medication lists, and placement status are accessible.
Preserves the complete discharge planning record including assessments, care plans, referrals, education documentation, and post-discharge follow-up for quality reporting and readmission reduction analysis.