Drug safety officer
Pharmacovigilance manager
Medical safety reviewer
Regulatory affairs specialist
Quality assurance lead
Chief medical officer

This process is used when the organization receives a report of a suspected adverse drug reaction from any source — healthcare providers, patients, clinical trials, published literature, regulatory authorities, or business partners. It applies when the report must be assessed against regulatory criteria for individual case safety reports (ICSRs) and when seriousness, causality, and expectedness must be determined to meet reporting obligations under ICH E2B, FDA, EMA, and other regulatory frameworks. It is common when safety scientists, medical reviewers, and regulatory teams must coordinate within strict timelines — typically 15 calendar days for serious and unexpected cases. Ideal for pharmaceutical companies, biotech firms, contract research organizations, and marketing authorization holders.
The pharmacovigilance case intake process typically involves safety intake staff who receive and log adverse event reports, drug safety officers who triage and assess initial seriousness, medical reviewers who evaluate causality and clinical significance, regulatory affairs specialists who determine reporting obligations and prepare submissions, and quality assurance who oversees process compliance.
On-time regulatory reporting by ensuring serious and unexpected cases are identified at intake and processed within mandatory timelines. Accurate case assessment because medical and safety review is structured into the intake flow rather than performed ad hoc after initial logging. Complete case documentation from the first report, reducing the need for follow-up queries that delay processing. Consistent triage classification across all reporting sources so no case is under-prioritized or misrouted. Audit-ready case records that demonstrate regulatory compliance with ICH, FDA, and EMA requirements for individual case safety report processing.
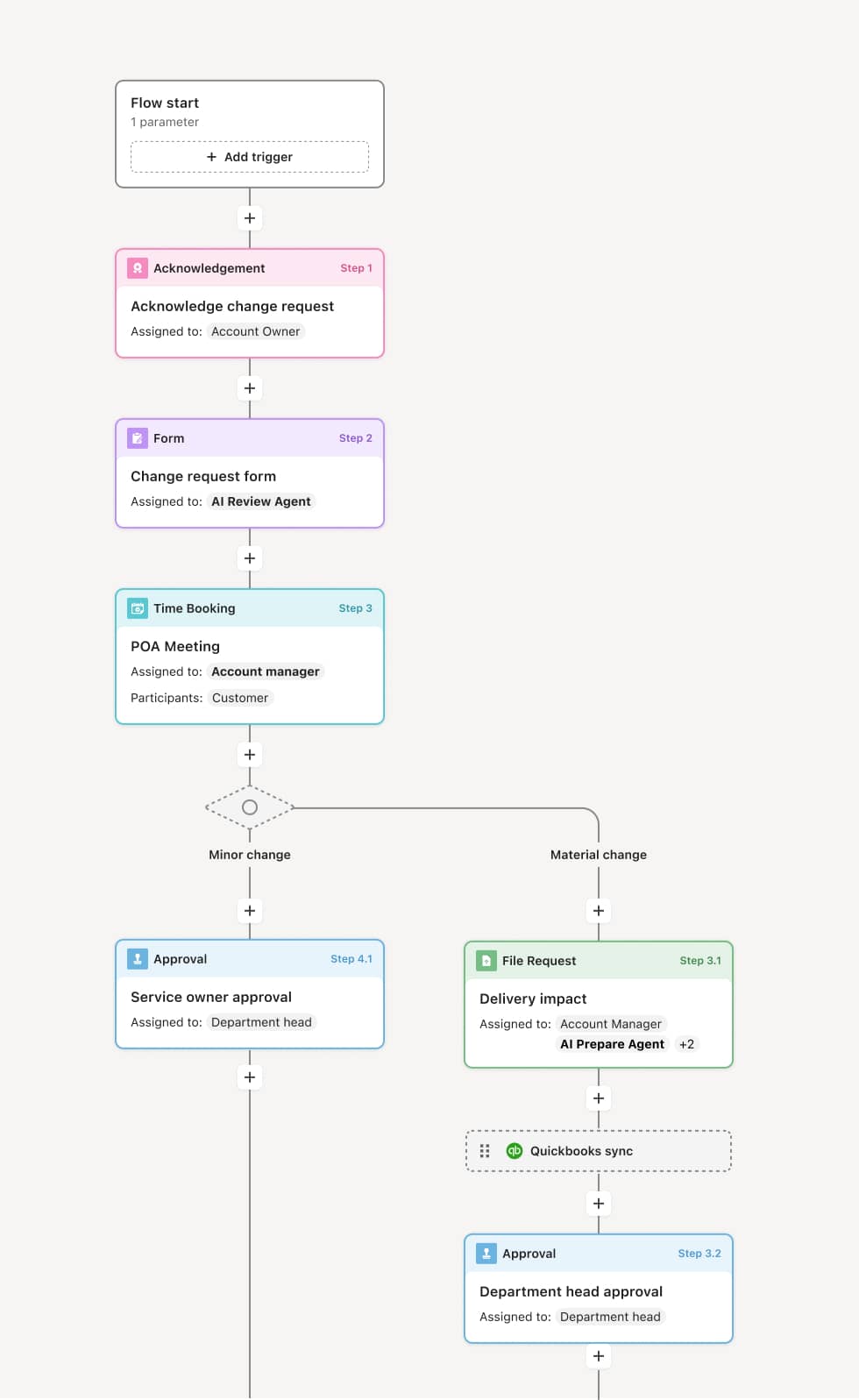
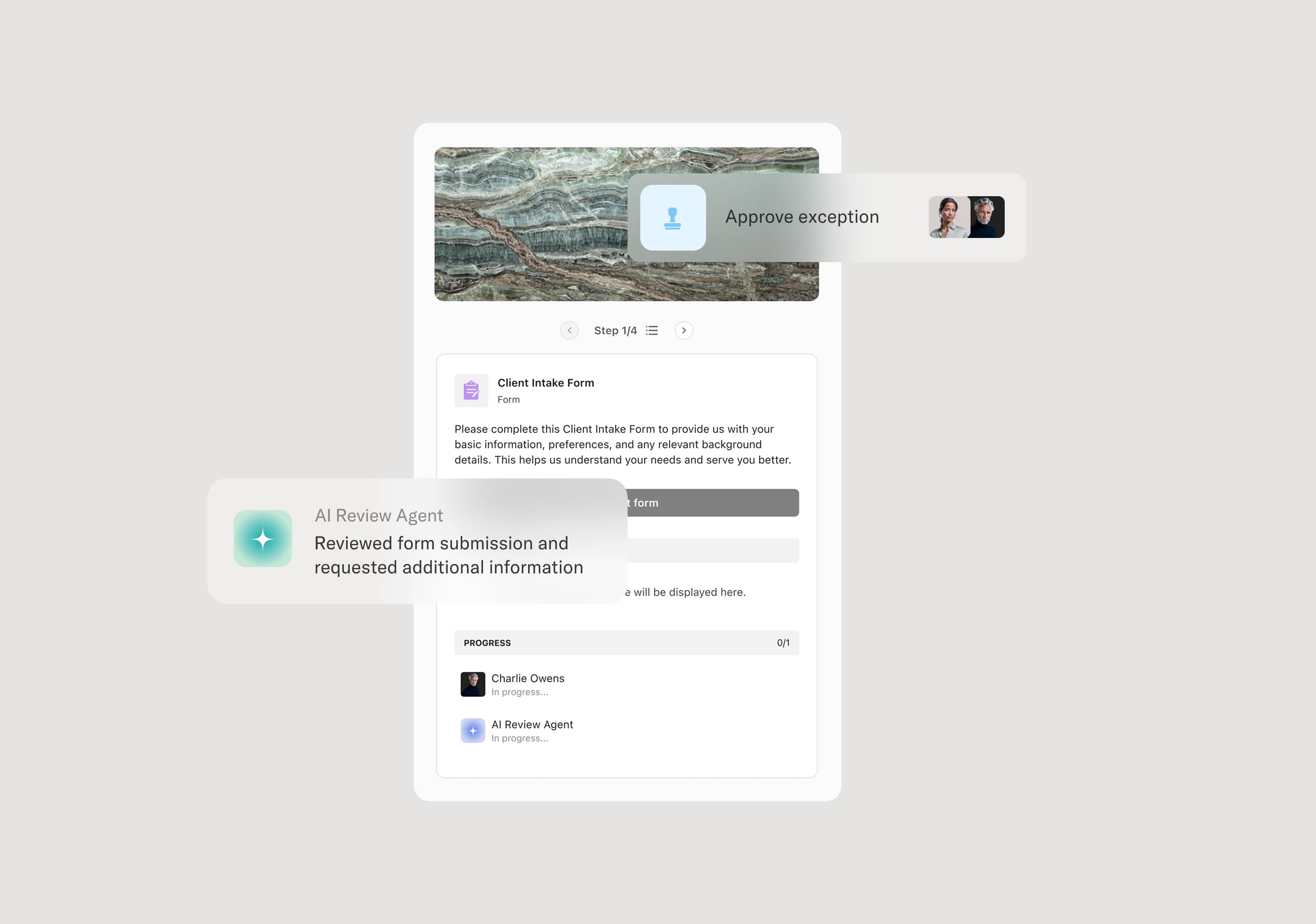
Your version of this process may vary based on roles, systems, data, and approval paths. Moxo’s flow builder can be configured with AI agents, conditional branching, dynamic data references, and sophisticated logic to match how your organization runs this workflow. The steps below illustrate one example.
Report receipt and case creation
The process begins when an adverse event report is received from any source — a healthcare professional, patient, clinical investigator, regulatory authority, or published literature. The report is logged with the minimum valid case elements: an identifiable reporter, an identifiable patient, a suspect product, and an adverse event. An AI Agent can assist by extracting structured data from unstructured report narratives, identifying the suspect product, and flagging missing minimum case elements.
Initial triage and seriousness assessment
The safety intake team triages the case to assess initial seriousness based on regulatory criteria — death, life-threatening, hospitalization, disability, congenital anomaly, or other medically important conditions. Serious cases are flagged for expedited processing. The triage also determines whether the case is solicited (from a clinical trial) or spontaneous, which affects reporting timelines and requirements.
Medical review and causality assessment
A medical reviewer or drug safety officer evaluates the clinical details, assesses the plausibility of a causal relationship between the product and the adverse event, and determines expectedness by comparing the event against the product’s reference safety information (core data sheet or product label). An AI Agent may compare the reported event against the known safety profile and flag unexpected reactions that trigger expedited reporting.
Regulatory reporting determination
Regulatory affairs determines the reporting obligations based on seriousness, expectedness, and the applicable regulatory framework. Serious and unexpected cases typically require expedited 15-day reporting to relevant health authorities. Expected serious cases may require periodic reporting. The appropriate report format (ICSR/E2B) and destination authorities are identified.
Case data quality review
Before submission, the case record is reviewed for data completeness, consistency, and accuracy. Missing information triggers follow-up requests to the original reporter. The case narrative is reviewed for clinical accuracy and clarity.
Submission and case tracking
The case is submitted to the applicable regulatory authorities within required timelines. Submission confirmation is recorded. The case enters the follow-up and lifecycle management phase for any additional information received.
This process commonly relies on inputs such as the adverse event report, patient demographics, product information, medical history, concomitant medications, and the reporter’s clinical assessment. It may be triggered by a report from a healthcare provider, patient, clinical trial site, literature review, or regulatory authority. Connected systems often include pharmacovigilance safety databases like Argus, ArisGlobal, or Veeva Vault Safety, regulatory submission gateways, and clinical trial management systems.
Key decision points include whether the report contains the minimum valid case elements for processing, the initial seriousness classification that determines processing timeline, whether the adverse event is expected or unexpected based on the product’s safety profile, and which regulatory authorities must receive the case report and within what timeframe.
Reports received without minimum case elements, requiring follow-up before the case can be processed and starting the regulatory clock late. Seriousness underestimated at triage, causing expedited cases to be processed on standard timelines and risking late regulatory submissions. Causality assessment delayed when medical reviewers are not engaged promptly, compressing the window for quality review and submission. Regulatory reporting obligations misidentified when cases are not assessed against all applicable frameworks and jurisdictions. Case documentation incomplete at submission, resulting in health authority queries and follow-up processing burden.
Orchestrates pharmacovigilance case intake from report receipt through regulatory submission across safety, medical, and regulatory teams in a single coordinated flow.
Routes cases based on seriousness and expectedness so expedited cases receive immediate attention and standard cases follow appropriate timelines.
AI Agents extract structured data from adverse event narratives at intake, identifying suspect products, adverse events, and seriousness indicators automatically.
Tracks regulatory submission deadlines within the workflow to ensure 15-day and periodic reporting obligations are met.
Connects to pharmacovigilance databases and regulatory gateways like Argus, ArisGlobal, and Veeva Vault Safety so case data flows directly into submission-ready formats.
Preserves the complete case processing record including triage, medical review, causality assessment, and submission documentation for audit, inspection, and signal detection.